Short stature is defined by being smaller for height compared to people who are the same age, sex, and ethnicity. This means that short stature affects about 2.5% of all children, as defined by being below the 2.3rd percentile on the growth chart. Poor height growth rate is when children fail to grow at least 2 inches per year, or are falling downward over height percentiles on the growth chart.
Poor growth rate and short stature can be signs of an underlying medical condition. All children with growth concerns should have, therefore, a thorough medical evaluation. Most children with short stature have a variation of normal growth, such as familial short stature (parents are smaller than average) or constitutional delay (“late bloomer”). These children are usually healthy and do not need medical treatment.
Growth hormone and thyroid hormone (called thyroxine or T4) help with height gain in children. Growth hormone is secreted by the pituitary gland, located in the brain at the level of our eyes. Thyroxine is secreted by the thyroid gland, located in the neck. The sex hormones estradiol and testosterone—from the ovaries and testes—lead to a growth “spurt” during puberty.
Certain endocrine problems cause a decrease in height growth rate and short stature, including:
Many medical conditions can lead to poor growth and short stature including:
Short stature itself does not usually cause any complications, except for functional problems associated with severe short stature. However, certain conditions associated with poor growth (such as hormone deficiency, illness or syndrome) may lead to other medical concerns independent of short stature.
The goal of a medical evaluation in a child with growth concerns is to figure out whether the growth is the result of a treatable medical condition or a normal variation, such as familial short stature or constitutional delay.
Children with familial short stature have parents with short stature as well. Their growth is stable, does not cross downwards over percentiles, and is appropriate for the parents’ heights. Constitutional delay is where children are “late bloomers.” They usually are shorter than most of the other children during childhood, enter puberty later than their peers, and then catch up to a height consistent with their parents during puberty. There is often a family history of late puberty.
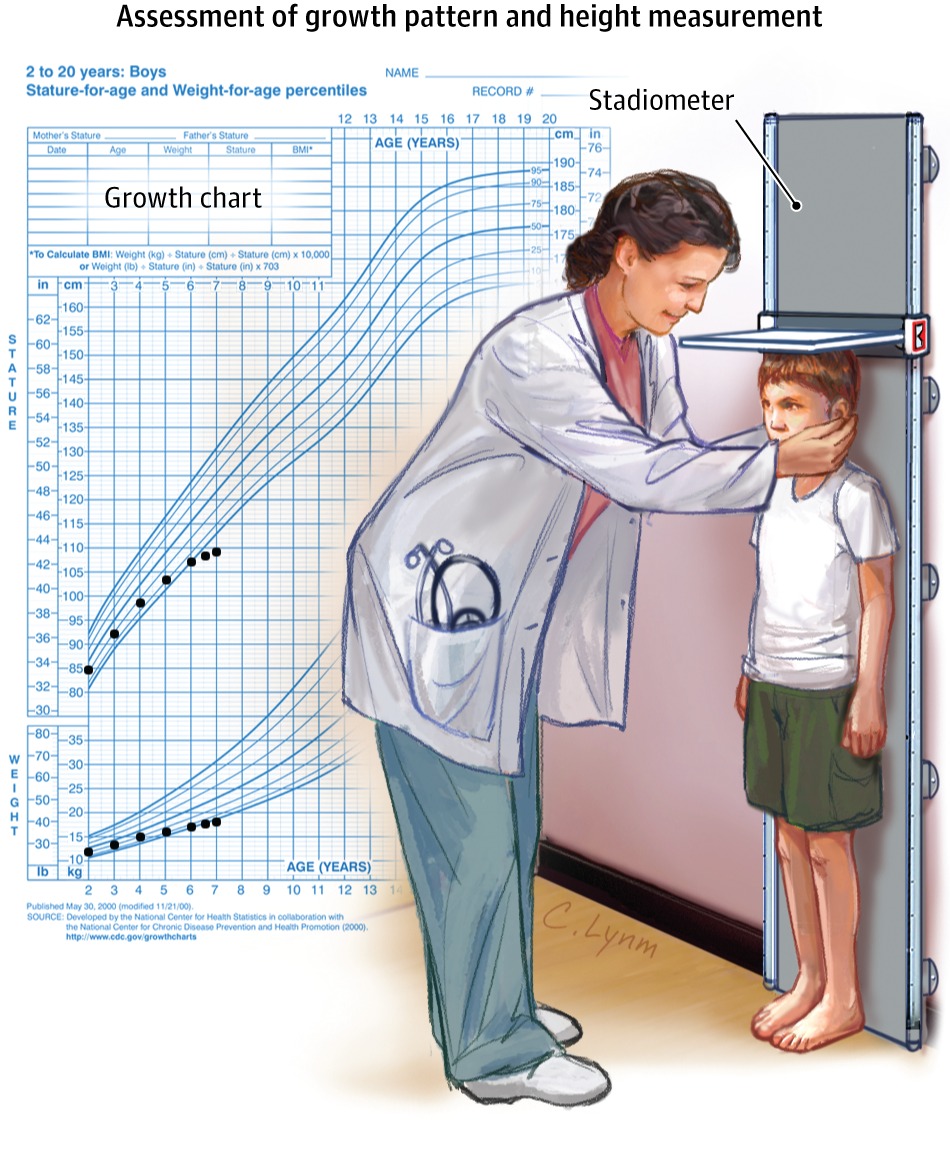
Medical providers track the child’s growth by plotting his/her height and weight on ethnicity-specific growth charts according to age (in years and months) and sex. Growth charts show how a child is growing compared to other children. Study of the growth chart determines the child’s pattern of growth and whether he/she needs additional evaluation. Short stature is diagnosed when height is below the normal ranges for age and sex (less than 23rd percentile)
A medical evaluation is done to identify a possible underlying medical cause that may affect growth. An evaluation of a child with growth concerns or short stature begins with a child’s medical history and a detailed family history, including parents’ heights and ages of puberty. Based on the results, the doctor can decide if additional labs or x-rays are needed. These medical examinations may include:
Blood Test: screen for kidney abnormalities, anemia, sensitivity to gluten (celiac disease), hypothyroidism, or abnormalities in growth hormone markers or puberty hormones.
Urine Analysis: This will be done if kidney abnormalities or urine infections are suspected.
Chromosome Assessment: This blood work may be recommended in girls to screen for Turner syndrome.
Bone Age: This is an x-ray of the left hand and wrist to determine the maturity of the bony growth plates to assess whether they are consistent with the child’s age and to see how much more time the child has to grow.
Additional endocrine testing may be needed to confirm diagnosis of growth hormone deficiency, including giving medications through an IV and testing growth hormone production over the next several hours. An MRI of the pituitary may be done in children with growth hormone deficiency to determine possible abnormalities of the pituitary gland.
Children with short stature may have no specific symptom beyond poor growth. Children with short stature because of familial short stature or constitutional delay are usually healthy. Children with growth hormone deficiency and no other hormonal abnormalities may have no specific symptoms.
If short stature is the result of an underlying systemic illness or syndrome, the child may present symptoms that relate to this specific condition. For example, children with inflammatory bowel disease may have frequent or bloody stools or poor weight gain. A child with a hypothyroidism may present with fatigue, feeling cold, constipation, dry skin and hair, and an enlarged thyroid (goiter) on physical examination.
Treatment and therapies
The treatment of short stature depends on the underlying cause. For example, if a child is found to have short stature because of hypothyroidism, thyroid hormone replacement will improve growth. For adolescents with growth slowing because of delayed or lack of puberty, treatment with sex hormones (estrogen or testosterone) will improve growth. Increasing calories can help a child with short statute because of undernutrition. For the rest of the cases, unfortunately, there is no specific food, diet, or exercise that can improve growth.
Growth hormone therapy is prescribed when:
Growth hormone therapy is generally considered safe for use in children. Possible short-term side effects are rare, but include a surgical condition causing hip pain (slipped capital femoral epiphyses [SCFE]), progression of scoliosis, fluid retention or edema (causing carpal tunnel syndrome or joint pain), increased growth of skin moles, or growth of adenoids and tonsils. Rarely, it can also cause persistent severe headaches (pseudotumor cerebrii), which resolves with discontinuation or lowering of growth hormone dose. Because it helps to promote growth, endocrinologists are cautious not to give too much growth hormone due to concern for possibly stimulating growth of any unknown cancers.
However, long term data to-date are very reassuring and do not suggest an increased risk of early death or malignancy, even in brain tumor survivors with growth hormone deficiency. The potential adverse effects in children are different from those in adults and should be discussed in detail before starting treatment. Not all children grow as hoped on growth hormone, so unmet expectations after use of a costly medication can be a negative outcome of treatment.
The outcome of children with short stature depends on the underlying causes.
Children who are treated with growth hormone for other indications (i.e., Turner, end- stage renal disease, SGA, idiopathic) usually experience an improvement in adult height but may not reach their parents’ heights.